
Insulin and Proinsulin in Type 2 Diabetes
Nov 9th 2021
Background
Diabetes is a chronic (long-lasting) health condition that affects how your body turns food into energy. More than 34 million people in the United States have diabetes, and 1 in 5 of them don't know they have it. More than 88 million US adults—over a third—have prediabetes, and more than 84% of them don't know they have it. Diabetes is the 7th leading cause of death in the United States (and may be underreported).
Most of the food you eat is broken down into sugar (also called glucose) and released into your bloodstream. When your blood sugar goes up, it signals your pancreas to release insulin. Insulin acts like a key to let the blood sugar into your body’s cells for use as energy.
If you have diabetes, your body either doesn’t make enough insulin or can’t use the insulin it makes as well as it should. When there isn’t enough insulin or cells stop responding to insulin, too much blood sugar stays in your bloodstream. Over time, that can cause serious health problems, such as heart disease, vision loss, and kidney disease.
There isn’t a cure yet for diabetes, but losing weight, eating healthy food, and being active can really help. Taking medicine as needed, getting diabetes self-management education and support, and keeping health care appointments can also reduce the impact of diabetes on your life.
A formal identification of type 2 diabetes relies primarily on the demonstration of glucose intolerance. However, in many patients, the disease may be well advanced at the time the finding is made. Such patients are already at an increased risk of cardiovascular disease and may require intervention.
Early detection of the disease is desirable since this provides an opportunity to initiate changes in lifestyle (eg diet and exercise) that can prevent or delay the onset of disease symptoms and in doing so impact significantly on the life quality for many as well as reducing treatment costs. This situation poses challenges at many levels, including diagnosis, monitoring and therapy. Better diagnosis can lead to earlier intervention. More rigorous monitoring can delay the onset of symptoms, while new treatments may offer better glycaemic control.
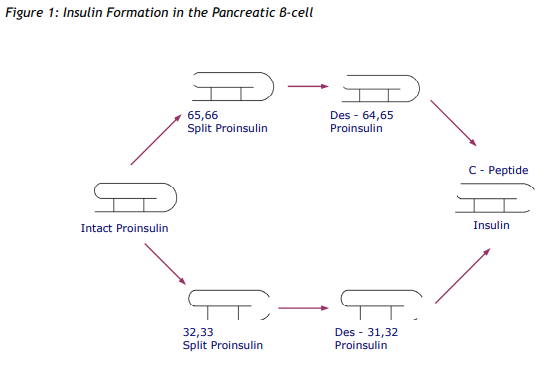
The hallmark of type 2 diabetes is insulin resistance. Additionally and, possibly as a consequence of this, significant changes in pancreatic βcell function occur from an early stage. Such changes can be assessed by measuring the release of insulin and its molecular precursors in the fasting state and in response to a glucose challenge. Insulin Processing Insulin is released from the β-cells of the Islets of Langerhans in the pancreas in response to the rise in blood glucose that follows a carbohydrate containing meal. It is synthesized initially as a high molecular weight precursor, proinsulin. This molecule is cleaved at two specific sites to yield two short polypeptide chains linked by two disulphide bridges (Figure 1). Under normal circumstances, only trace amounts of “intact” proinsulin or the intermediate metabolites of processing (“split” proinsulins) survive to be released into peripheral blood. When the pancreas is subjected to repeated or increased stimulation by glucose, as occurs in insulin resistance, this molecular processing becomes less efficient and increasing proportions of intact and split proinsulins appear in peripheral blood.
Early Detection of Type 2 Diabetes
While the risk of becoming diabetic risk can be calculated on the basis of lifestyle markers, it has not yet been possible to identify at-risk subjects on the basis of biochemical abnormalities. Classically, a diagnosis of diabetes is made on the basis of a fasting plasma glucose >7.0 mmol/l and/or a plasma glucose >11.1 mmol/l two hours after a 75g oral glucose load.
Early in 2010, the American Diabetes Association (ADA) recommended the use of glycosylated haemoglobin measurement (HbA1c) both for the diagnosis of type 2 diabetes (HbA1c ≥ 6.5%) and also as a potential screening test for the early diabetic subject (HbA1c 5.7-6.4%). Data produced within the subsequent year have done little to support this latter proposal, one study reporting that an HbA1c within the range 5.7-6.4% detected only 23% of at-risk individuals whereas 59% were found to have impaired glucose tolerance (1). The main attraction of HbA1c as a screening test is that it precludes the inconvenience of obtaining fasting blood samples.
In the last 20 years, several studies have suggested that changes in pancreatic β-cell function may indicate a pre-diabetic situation. In 1999, Wareham et al (2) published data on a 4.5 year population based longitudinal study in which they demonstrated an association between elevated fasting proinsulin concentrations at the beginning of the study and a subsequent progression to diabetes. This predictive value of proinsulin measurement has been confirmed in other studies (3, 4).
Insulin Resistance
A quantitative measure of insulin resistance can be helpful in designing appropriate therapy and predicting outcome in patients with type 2 diabetes. The accepted methods for determining insulin resistance, such as the euglycaemic clamp or intravenous glucose tolerance test are expensive and time consuming and so inappropriate for routine investigation. A homeostatic model analysis (HOMA), based on the relationship between fasting insulin and fasting glucose, has been widely used in epidemiological studies as an index of insulin resistance. Overall, the HOMA score correlates well with euglycaemic clamp results, though it is recognized to be of relatively little value in the individual subject because of its low specificity (5). Recent studies have confirmed that circulating proinsulin is a highly specific marker of insulin resistance (6). Earlier work in Japan had demonstrated that while the sulphonylurea glyclazide was effective in improving glycaemic control in diabetics, a thiazolidinedione (pioglitazone) was equally effective but, in addition, produced a significant reduction in proinsulin levels (7). It is logical to conclude that proinsulin measurement in individual diabetic patients provides a reliable index of insulin resistance. In addition to its role as an early indicator of the disease, it may also provide an important marker for selecting and monitoring an appropriate therapeutic regime.
References
1. Lorenzo C et al. A1C between 5.7 and 6.4% as a marker for identifying pre-diabetes, insulin sensitivity and secretion, and cardiovascular risk factors. Diabetes Care 2010; 33: 2104-2109.
2. Wareham NJ et al. Fasting proinsulin concentrations predict the development of type 2 diabetes. Diabetes Care 1999; 22: 262-270.
3. Hanley AJ et al. Increased proinsulin levels and decreased acute insulin response independently predict the incidence of type 2 diabetes in the insulin resistance atherosclerosis study. Diabetes 2002; 51: 1263-1270.
4. Zethelius B et al. Insulin resistance, impaired early insulin response and insulin propeptides as predictors of the development of type 2 diabetes: a population-based, 7-year follow-up study in 70-year-old men. Diabetes Care 2004; 27 1433-1438.
5. Bonora E et al. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity. Diabetes Care 2000; 23: 57-63.
6. Pfützner A et al. IRIS II study: intact proinsulin is confirmed as a highly specific indicator for insulin resistance in a large cross-sectional study design. Diabetes Technology & Therapeutics 2005; 7: 478-486.
7. Kubo K. Effect of pioglitazone on blood proinsulin levels in patients with type 2 diabetes mellitus. Endocrine Journal 2002; 49: 323-328.