Titin
May 29th 2026
Titin, also known as connectin, is a giant protein of ~3,800 kDa and is a component of the sarcomere, the building block of muscle. The N-terminal portion of titin is ~26kDa.1 Immuno-Biological Laboratories Co., Ltd., Japan, organized a conference where “Urinary Titin as a Biomarker of Muscle Injury” was a topic. A summary of this presentation follows.
N-titin is known to be a marker of muscle injury and muscle atrophy. Muscles contract by sliding actin along myosin while titin is thought to act as a spring to restore the contracted muscle. N-Titin was identified by proteome analysis as a peptide present in large amounts in the urine of patients with Duchenne muscular dystrophy (DMD).2
In 2016, Maruyama and colleagues developed an ELISA kit to measure urinary N-titin. Measurement range: 46.9~3,000 pmol/L with a detection limit: 27.9 pmol/L.3 N-titin assays have been used in many research projects.
Numerous papers have been published on the relationship between Titin and diseases or physiological conditions. On the left, are the diseases and physiological conditions with the right column containing the PubMed IDs:
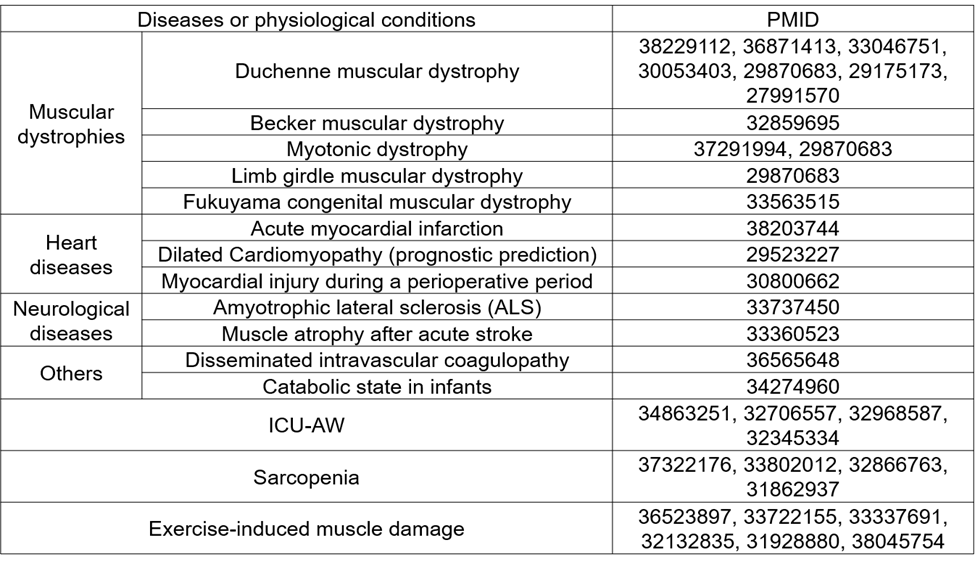
As one can see, urinary N-titin levels are associated with a variety of diseases or physiological conditions dealing with muscle damage or muscle atrophy. A few of these relationships are discussed in more detail.
- Duchenne muscular dystrophy (DMD)
DMD is a muscular dystrophy with a frequency of about 1 in ~3,000 children. When affected by this disease, muscle weakness begins around age 4. The child becomes wheelchair-bound after age 10, later develops respiratory failure and cardiomyopathy. The average life expectancy is 29 years. The disease is caused by a mutation of the dystrophin gene on the X chromosome with highest prevalence in males. The disease is suspected to be caused by high creatine kinase levels and may be diagnosed by genetic testing or muscle biopsy. Currently, there is no specific treatment for this disease, but new drugs, such as exon skipping drugs, are in development.
In a study where DMD patients were diagnosed by genetic testing, the median value of urinary N-titin (corrected by creatine levels) in DMD patients was vastly higher than that of healthy individuals.4 Similarly, Awano et al., reported measuring urinary N-titin was extremely accurate as a diagnostic marker for identifying DMD.5
Blood sampling may be difficult in young children. It is beneficial to diagnose DMD at a young age to allow therapy to begin before severe symptoms onset. Minimally invasive urine testing is a great advantage for screening DMD in children.6
Research has also utilized a DMD mouse model. DMD-null mice had much higher levels of N-titin than wild type control mice (untreated normal mice). DMD mice transfected with the dystrophin gene, resulted in lower levels of urinary N-titin than DMD-null mice, indicating that the inserted gene successfully compensates for the disrupted dystrophin gene in DMD mice.
Plasma creatine kinase (CK) is used as a marker of DMD. DMD-null mice exhibited higher levels of plasma CK than wild type control mice. Similar to what was seen with urinary N-titin determinations, mice with the inserted dystrophin gene had reduced plasma CK levels. The authors noted that urinary N-titin may be a more sensitive DMD biomarker than plasma CK.7
- Acute Myocardial Infarction (AMI)
N-titin is excreted in urine as a result of skeletal muscle destruction. Cardiac muscle also contains titin, so that N-titin may also function as a marker for myocardial infarction.
AMI is a condition where coronary arteries of the heart become occluded by thrombus or plaque, preventing sufficient oxygen and nutrients resulting in necrosis of the myocardium. This disease ranks as the second leading cause of mortality among Japanese people. It is reported to be fatal in 5-10% of cases even when patients receive treatment at a hospital. To save lives, catheterization should be performed as early as possible after the onset of disease as a longer time to treatment results in higher mortality.
To diagnose AMI, troponin T is a useful biomarker, but this marker may also be elevated in renal disease and should be determined by continuous measurements. Another biomarker may be better.
Urinary N-titin was measured in 83 patients with suspected AMI. Of these 83 patients, 51 were diagnosed with AMI. Urinary N-titin levels were significantly higher in AMI-diagnosed patients than non-AMI patients when measured after symptom onset at 3 or more hours. Urinary titin levels were vastly higher in patients who died during hospitalization than discharged AMI-patients. Urinary N-fragment titin may serve as an effective early diagnostic biomarker of AMI while also having predictive prognosis value.8
- Intensive Care Unit-Acquired Weakness (ICU-AW)
Muscle atrophy occurs in patients admitted to the intensive care unit (ICU). The disease strikes 40-50% of ICU-admitted patients. Most patients develop the disease within 3 days of ICU admission, with a 13-21% loss of muscle mass within 7 days. This muscle mass loss is associated with long-term decline in physical function and mortality after ICU-discharge. Muscle atrophy results from increased muscle protein catabolism and decreased anabolism. However, the detailed mechanism is not known. The diagnosis of the disease is often made by muscle strength assessment called the Medical Research Council (MRC) score. Patients with non-ICU-AW exhibited lower levels on urinary N-titin corrected for creatine than did ICU-AW patients. ICU-AW patients had higher N-titin levels from day 1 and continued to have higher levels until day 7.9
Evaluation by biomarkers has not been established for ICU-AW. Thus, a biomarker to aid in diagnosing ICU-AW is an unmet medical need. Urinary N-titin may be useful in this regard. Two studies examined determination accuracy of ICU-AW by N-Titin levels looking at Area Under the Curve (AUC) plotting sensitivity against specificity. The closer the AUC value is to 1, the higher the diagnostic accuracy.
Nakanishi et al. calculated the AUCs for cumulative urinary N-titin levels from day 1 to day 7 of ICU admission and for the urinary N-titin level on day 2 of admission. The AUCs were 0.78 (95% CI, 0.61-0.95) and 0.75 (95% CI, 0.56-0.94), respectively.10
Nakano et al., reported AUCs calculated for urinary N-titin was 0.810 (95% CI, 0.688-0.931) while using serum creatinine kinase levels gave 0.654 (95% CI, 0.494-0.814), indicating use of urinary N-titin levels as a diagnostic marker was more accurate than using serum CK for diagnosis of ICU-AW.9 Urinary N-titin may be useful in diagnosing ICU-AW.
- Sarcopenia
Sarcopenia refers to the decrease in muscle mass throughout the body primarily due to aging and the accompanying loss of muscle strength and physical function. In recent years, sarcopenia has been internationally recognized as a disease that should be treated with 16-29% of individuals over 80 years being affected.
Sarcopenia may be classed as primary sarcopenia, which is caused by aging and secondary sarcopenia, which has causes other than aging, such as disease or malnutrition. The diagnosis is based on walking speed, grip strength, skeletal muscle mass, or other indicators such as skeletal muscle mass index (muscle mass/height squared) or sarcopenia index (muscle mass/BMI). Biomarkers that enable simple and objective diagnosis are needed.
Here are two examples of analyzing urinary N- titin levels in secondary sarcopenia. In the first study, urinary N-titin levels were measured in 39 preoperative patients with malignancies. The mean urinary N-titin levels of 8 sarcopenia patients and 31 non-sarcopenia patients were 8.3 and 4.9 pmol/mg Cr, respectively, indicating that N-titin was significantly higher (P=0.04) in sarcopenia patients.
The authors further analyzed urinary N-titin levels in patients with gastrointestinal malignancies and patients with hepatobiliary-pancreatic malignancies and found that patients with gastrointestinal malignancies and patients with hepatobiliary-pancreatic malignancies had urinary N-titin levels of 6.1 pmol/mg Cr and 5.2 pmol/mg Cr, respectively. There was no significant difference between the two groups, but patients with gastrointestinal malignancies had slightly higher urinary N-titin levels.
Patients with malignancies generally have a decreased appetite due to a symptom called cachexia. The higher N-titin levels of patients with gastrointestinal malignancies also suggested that urinary N-titin levels may be related to the nutritional status of the patients. A negative correlation was found between urinary N-Titin levels and indicators of nutritional status (albumin, prealbumin, and BMI) in preoperative tumor patients.
Urinary N-Titin levels may be useful as a marker of sarcopenia, which may be caused by low nutritional status in gastrointestinal and other malignancies.11
The second study examined N-titin levels in patients with sarcopenia resulting from non-alcoholic fatty liver disease (NAFLD). NAFLD is now also known as metabolic dysfunction-associated steatotic liver disease (MAFLD). MAFLD occurs in an over-nutrition state, such as may be seen in individuals with metabolic syndrome, diabetes, and obesity.
For this study, 153 MAFLD individuals and 100 individuals without MAFLD, obesity or diabetes mellitus (non-MAFLD) were enrolled. MAFLD subjects had higher N-titin levels than non-MAFLD subjects. Urinary levels of titin-N fragment reflected skeletal muscle deterioration and functional decline. Furthermore, N-titin levels were closely associated with hepatic pathological conditions in MAFLD individuals.12
- Exercise-induced muscle damage
Exercise-induced muscle damage refers to muscle damage caused by unfamiliar exercise or other factors, resulting in symptoms such as muscle weakness and muscle pain. Severe muscle damage causes destruction of muscle fibers and inflammation that may last for 30 days or more.
Exercise may be classified as either concentric exercise, in which muscles are contracted, or eccentric exercise, in which muscles are stretched. Exercise-induced muscle damage is more likely to occur after eccentric exercise.
SOR, a numerical measure of muscle soreness, and ROM, a measure of joint range of motion, are used as indicators of exercise-induced muscle damage. Creatine kinase is also known to be a useful biomarker for exercise-induced muscle damage but requires blood sampling. Biomarkers that utilize non-invasive samples are needed.
As you may have experienced, muscle soreness occurs after intense exercise. However, muscle soreness is reduced when the same exercise is repeated afterward. This is called the repeated bout effect.
In this study, eight male participants performed 30 eccentric exercises of elbow flexion, Bout1, with urine samples were collected over time.
Two weeks later, they performed the same exercise routine, Bout2, with urine samples collected in the same manner.
Muscle soreness in Bout1, peaked 24-48 hours after exercises. The level of muscle soreness decreased following Bout2. Muscle soreness is reduced after the second exercise (Repeated bout effect). This phenomenon was also strongly reflected in urinary N-Titin levels with N-titin levels being greatly reduced after Bout2. This experiment demonstrates that urinary N-titin is an excellent biomarker for exercise-induced muscle damage.13
In summary, there are many potential uses for urinary N-titin measurement:
N-titin is a highly accurate diagnostic marker for DMD and is more sensitive than creatine kinase. DMD may be diagnosed in infants, for whom blood sampling may be difficult. N-titin has the advantage of being measured in non-invasive urine specimens. In addition, N-titin may be useful as a monitoring marker for effectiveness of DMD drugs.
N-titin may serve as a diagnostic marker for ICU-AW, which has a high incidence in ICU patients. There currently is no established evaluation procedure for ICU-AW. N-titin determination may meet an unmet medical need, as it is more accurate than creatine kinase for diagnosis and prognosis of ICU-AW.
N-titin may act as an adjunctive diagnostic marker for cardiac and cranial nerve disease. There is also potential as a prognostic marker for cardiac diseases (acute myocardial infarction, dilated cardiomyopathy, etc.) and cranial nerve diseases (ALS, stroke, etc.). N-titin determinations may be utilized in emergency medicine, especially if point-of-care testing becomes available.
N-titin may be utilized as a diagnostic marker for sarcopenia/frailty. Sarcopenia/frailty impact quality of life. Reducing sarcopenia/frailty may extend the healthy life span. N-titin determination could potentially be an objective biomarker of physical function.
N-titin may be an indicator of the effectiveness of dietary therapy and rehabilitation for both sarcopenia/frailty and ICU-AW. It may also be useful in evaluating supplements and functional foods as therapies.
The determination of urinary N-titin may be used in sports medicine research as a biomarker that accurately reflects degree of muscle damage. A point of care test could aid in athlete training. The results from N-titin testing may help develop functional foods and supplements to prevent injuries and accelerate recovery from muscle damage.
The future of N-titin determination offers a wealth of possibilities. It will be interesting to see how this biomarker will be utilized, perhaps in studies examining incretin-mimetic drug and muscle loss. IBL-America offers Human Titin N-Fragment and Mouse Titin N-Fragment urine and serum sandwich ELISA kits. Please visit the IBL-America website (IBL America Online Store) for more information on these and our other offerings.
Citations
1Nakanishi N et al. J Clin Med. 2021. PMID: 33561946
2Rouillon J et al. Neuromuscul Disord. 2014. PMID: 24813925
3Maruyama N et al. Sci Rep. 2016. PMID: 27991570
4Boehler JF et al. Skelet Muscle. 2024. PMID: 38229112
5Awano H et al. Clin Chim Acta. 2018. PMID: 29175173
6Matsuo M et al. Clin Chim Acta. 2018. PMID: 30053403
7Hiramuki Y et al. Sci Rep. 2025. PMID: 39805937
8Arase M et al. Int J Mol Sci. 2024. PMID: 38203744
9Nakano H et al. Am J Respir Crit Care Med. 2021. PMID: 33030965
10Nakanishi N et al. Crit Care Med. 2020. PMID: 32706557
11Miyoshi K et al. Nutrition. 2020. PMID: 32866763
12Oshida N et al. Sci Rep. 2019. PMID: 31862937
13Yamaguchi S et al. J Sci Med Sport. 2019. PMID: 31928880